What is the most important information I should know about TYMLOS?
TYMLOS may cause serious side effects including: Possible bone cancer (osteosarcoma). During animal drug testing, TYMLOS caused some rats to develop a bone cancer called osteosarcoma. It is not known if people who take TYMLOS will have a higher chance of getting osteosarcoma.
- Tell your healthcare provider right away if you have pain in your bones, pain in any areas of your body that does not go away, or any new or unusual lumps or swelling under your skin that is tender to touch.
Do not take TYMLOS: if you had an allergic reaction to abaloparatide or any of the other ingredients in TYMLOS. The inactive ingredients in TYMLOS are phenol, sodium acetate trihydrate, acetic acid, and water for injection.
Before you take TYMLOS, tell your healthcare provider about all of your medical conditions, including if you:
- have Paget’s disease of the bone or other bone disease.
- have or have had any of the following: cancer in your bones; radiation therapy involving your bones; too much calcium in your blood; or an increase in your parathyroid hormone (hyperparathyroidism).
- will have trouble injecting yourself with the TYMLOS pen and do not have someone who can help you.
- are pregnant or plan to become pregnant, because TYMLOS is not for pregnant women, or if you are breastfeeding or plan to breastfeed. It is not known if TYMLOS passes into your breast milk; you should not take TYMLOS and breastfeed.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
What are the possible side effects of TYMLOS?
TYMLOS can cause serious side effects including:
- Decrease in blood pressure when you change positions. Some people may feel dizzy, have a faster heartbeat, or feel lightheaded soon after the TYMLOS injection is given. These symptoms generally go away within a few hours. Take your injection of TYMLOS in a place where you can sit or lie down right away if you get these symptoms. If your symptoms get worse or do not go away, stop taking TYMLOS and call your healthcare provider.
- Increased blood calcium (hypercalcemia). TYMLOS can cause some people to have a higher blood calcium level than normal. Your healthcare provider may check your blood calcium before you start and during your treatment with TYMLOS. Tell your healthcare provider if you have nausea, vomiting, constipation, low energy, or muscle weakness. These may be signs there is too much calcium in your blood.
- Increased urine calcium (hypercalciuria). TYMLOS can cause some people to have higher levels of calcium in their urine than normal. Increased calcium may also cause you to develop kidney stones (urolithiasis) in your kidneys, bladder, or urinary tract. Tell your healthcare provider right away if you get any symptoms of kidney stones which may include pain in your lower back or lower stomach area, pain when you urinate, or blood in your urine.
The most common side effects of TYMLOS in women with postmenopausal osteoporosis include: dizziness, nausea, headache, fast heartbeat, feeling tired (fatigue), upper stomach pain, and spinning feeling (vertigo).
The most common side effects of TYMLOS in men with osteoporosis include: redness at injection site, dizziness, joint pain, swelling at injection site, pain at injection site, bruising, abdominal bloating, diarrhea, nausea, abdominal pain, and bone pain.
These are not all the possible side effects of TYMLOS. Call your doctor for medical advice about side effects. You may report side effects to the FDA at 1-800-FDA-1088.
How should I use TYMLOS?
- Read the complete Instructions for Use (opens in a new tab) provided with your medicine.
- If you take more TYMLOS than prescribed you may experience symptoms such as muscle weakness, low energy, headache, nausea, dizziness (especially when getting up after sitting for a while), and a faster heartbeat. Stop taking TYMLOS and call your healthcare provider right away.
- You should not use TYMLOS for more than 2 years over your lifetime.
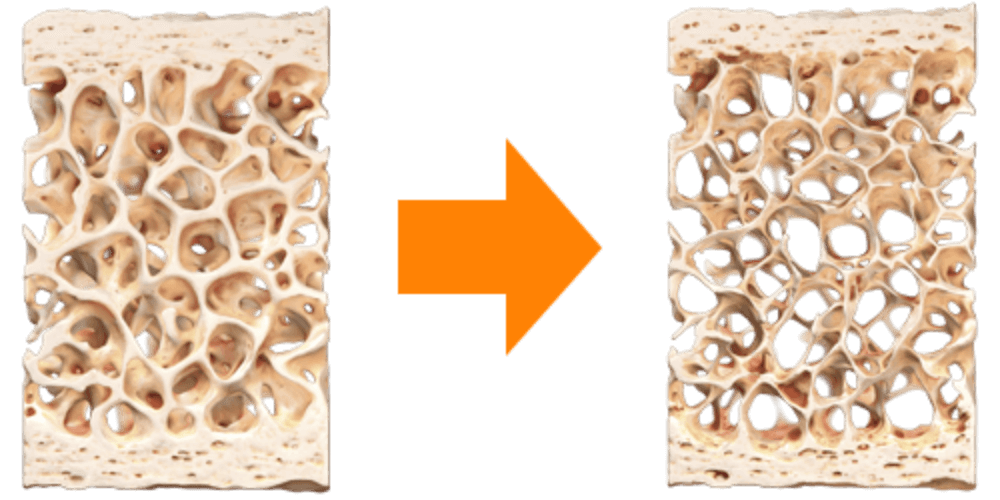
 TYMLOS can help you stand up to
TYMLOS can help you stand up to